

INVESTIGATIVE REPORT - Part Two: the FDA, a foreign regulatory authority in Canada?

PART TWO – the FDA, a foreign regulatory authority in Canada?
Section C.08.009.03(1)(a)(i)(B) in Division 8 the Canadian Food and Drug Regulation — Pre-positioning of Designated COVID-19 Drugs — states that “the holder of an establishment licence may import a designated COVID-19 drug” if:
An application has been submitted to a foreign regulatory authority to authorize the sale of the designated COVID-19 drug,
Canada’s Food and Drug Regulation defines a foreign regulatory authority (e.g., the FDA) as:
A government agency or other entity outside Canada that has a legal right to control the manufacturing, use or sale of drugs within its jurisdiction and that may take enforcement action to ensure that drugs marketed within its jurisdiction comply with the applicable legal requirements.
Consequently, it is necessary to take a careful look at what the FDA has been up to. As noted in the preamble to Part One, on August 23, 2021, the FDA directed two (2) separate letters to Pfizer Inc. and BioNTech GmbH regarding the manufacture and sale of the original BioNTech and “new” COMIRNATY labeled Covid-19 drugs, and it is to these two letters that we now turn.
But before we do, take the time to carefully read the following caption from — Will covid-19 vaccines save lives? Current trials aren’t designed to tell us — published in the British Medical Journal on October 21, 2020:
… the current phase III trials are not actually set up to prove either (table 1). None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.
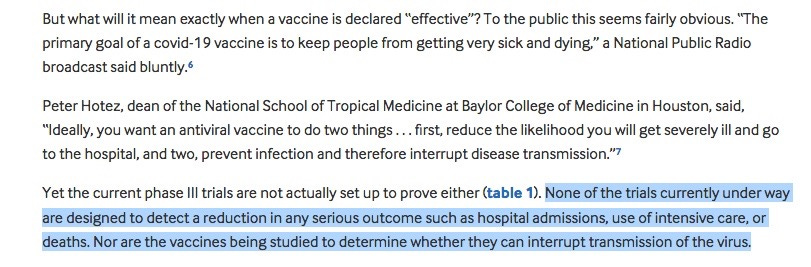
Figure 2: “Will covid-19 vaccines save lives? Current trials aren’t designed to tell us” - BMJ2020; 371 doi: https://doi.org/10.1136/bmj.m4037 (Published 21 October 2020)
FDA Letter One - to Pfizer Inc.:
On August 23, 2021 the FDA sent this letter (“Letter One”) to Pfizer Inc. Collegeville, PA, dated August 23, 2021, Attention: Ms. Elisa Harkins. On page 1 of this letter, at paragraph two, the FDA wrote:
On December 11, 2020, the Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for emergency use of Pfizer-BioNTech COVID‐19 Vaccine for the prevention of COVID-19 for individuals 16 years of age and older pursuant to Section 564 of the Act.
On page 2, paragraph one, the FDA advises:
On August 23, 2021, FDA approved the biologics license application (BLA) submitted by BioNTech Manufacturing GmbH for COMIRNATY (COVID-19 Vaccine, mRNA) for active immunization to prevent COVID-19 caused by SARS-CoV-2 in individuals 16 years of age and older. The FDA (last) reissued the letter of authorization on … August 12, 2021.
In paragraph three, page 2, the FDA goes on to state that:
COMIRNATY (COVID-19 Vaccine, mRNA) is the same formulation as the Pfizer- BioNTech COVID-19 Vaccine and can be used interchangeably with the Pfizer-BioNTech COVID-19 Vaccine to provide the COVID-19 vaccination series.
And in footnote 8, the FDA added:
The licensed vaccine (Comirnaty) has the same formulation as the EUA-authorized vaccine (BioNTech) and the products can be used interchangeably to provide the vaccination series without presenting any safety or effectiveness concerns. The products are legally distinct with certain differences that do not impact safety or effectiveness.
FDA Letter Two - to BioNTech Manufacturing GmbH:
Also on August 23, 2021, the FDA directed this letter (“Letter Two”) to Mr. Amit Patel, BioNTech GmbH New York, NY. In this letter FDA granted Pfizer-BioNTech's COMIRNATY Covid-19 a 'Biologics License Application' (BLA).
Now licensed (aka “approved”) COMIRNATY is not protected by an EUA liability shield from any lawsuits that result from any death or injury it might cause. Meanwhile, we await completion of 13 studies of COMIRNATY to evaluate its safety, details on 11 of which are listed below.
Abridged List of Pfizer-BioNTech Comirnaty Covid-19 Vaccine Studies:
For parents, Studies 1, 2, 3, and 5 may be considered the most significant in the near term. Study 10 concerns “Pregnancy and Infant Outcomes”. Study 7, “a prospective cohort study with at least 5 years of follow-up for potential long-term sequelae of myocarditis after vaccination”, is not due to be submitted to the FDA until May 31, 2027.
1. Deferred pediatric Study C4591001 to evaluate the safety and effectiveness of COMIRNATY in children 12 years through 15 years of age.
Final Protocol Submission: October 7, 2020
Study Completion: May 31, 2023
Final Report Submission: October 31, 2023
2. Deferred pediatric Study C4591007 to evaluate the safety and effectiveness of COMIRNATY in infants and children 6 months to <12 years of age.
Final Protocol Submission: February 8, 2021
Study Completion: November 30, 2023
Final Report Submission: May 31, 2024
3. Deferred pediatric Study C4591023 to evaluate the safety and effectiveness of COMIRNATY in infants <6 months of age.
Final Protocol Submission: January 31, 2022
Study Completion: July 31, 2024
Final Report Submission: October 31, 2024
On page 6 the letter (Letter Two) the FDA advises BioNTech Manufacturing GmbH:
We have determined that an analysis of spontaneous postmarketing adverse events reported under section 505(k)(1) of the FDCA will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis. [emphasis added]
Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA is not sufficient to assess these serious risks.” [emphasis added]
Therefore, based on appropriate scientific data, we have determined that you are required to conduct the following studies.”
4. Study C4591009, entitled “A Non-Interventional Post-Approval Safety Study of the Pfizer-BioNTech COVID-19 mRNA Vaccine in the United States,” to evaluate the occurrence of myocarditis and pericarditis following administration of COMIRNATY.
We acknowledge the timetable you submitted on August 21, 2021, which states that you will conduct this study according to the following schedule:
Final Protocol Submission: August 31, 2021
Monitoring Report Submission: October 31, 2022
Interim Report Submission: October 31, 2023
Study Completion: June 30, 2025
Final Report Submission: October 31, 2025
5. Study C4591021, entitled “Post Conditional Approval Active Surveillance Study Among Individuals in Europe Receiving the Pfizer-BioNTech Coronavirus Disease 2019 (COVID-19) Vaccine,” to evaluate the occurrence of myocarditis and pericarditis following administration of COMIRNATY.
We acknowledge the timetable you submitted on August 21, 2021, which states that you will conduct this study according to the following schedule:
Final Protocol Submission: August 11, 2021
Interim Report 1 Submission: March 31, 2022
Interim Report 2 Submission: September 30, 2022
Interim Report 3 Submission: March 31, 2023
Interim Report 4 Submission: September 30, 2023
Interim Report 5 Submission: March 31, 2024
Study Completion: March 31, 2024
Final Report Submission: September 30, 2024
6. Study C4591021 substudy to describe the natural history of myocarditis and pericarditis following administration of COMIRNATY.
We acknowledge the timetable you submitted on August 21, 2021, which states that you will conduct this study according to the following schedule:
Final Protocol Submission: January 31, 2022
Study Completion: March 31, 2024
Final Report Submission: September 30, 2024
7. Study C4591036, a prospective cohort study with at least 5 years of follow-up for potential long-term sequelae of myocarditis after vaccination (in collaboration with Pediatric Heart Network).
We acknowledge the timetable you submitted on August 21, 2021, which states that you will conduct this study according to the following schedule:
Final Protocol Submission: November 30, 2021
Study Completion: December 31, 2026
Final Report Submission: May 31, 2027
8. Study C4591007 substudy to prospectively assess the incidence of subclinical myocarditis following administration of the second dose of COMIRNATY in a subset of participants 5 through 15 years of age.
We acknowledge the timetable you submitted on August 21, 2021, which states that you will conduct this assessment according to the following schedule:
Final Protocol Submission: September 30, 2021
Study Completion: November 30, 2023
Final Report Submission: May 31, 2024
9. Study C4591031 substudy to prospectively assess the incidence of subclinical myocarditis following administration of a third dose of COMIRNATY in a subset of participants 16 to 30 years of age.
We acknowledge the timetable you submitted on August 21, 2021, which states that you will conduct this study according to the following schedule:
Final Protocol Submission: November 30, 2021
Study Completion: June 30, 2022
Final Report Submission: December 31, 2022
10. Study C4591022, entitled “Pfizer-BioNTech COVID-19 Vaccine Exposure during Pregnancy: A Non-Interventional Post-Approval Safety Study of Pregnancy and Infant Outcomes in the Organization of Teratology Information Specialists (OTIS)/Mother To Baby Pregnancy Registry.”
Final Protocol Submission: July 1, 2021
Study Completion: June 30, 2025
Final Report Submission: December 31, 2025
11. Study C4591007 substudy to evaluate the immunogenicity and safety of lower dose levels of COMIRNATY in individuals 12 through <30 years of age.
Final Protocol Submission: September 30, 2021
Study Completion: November 30, 2023
Final Report Submission: May 31, 2024
After reviewing this long list of clinical studies, no less than six of which are to prospectively assess “known serious risks” already identified by the FDA, and all of which are years away from completion, might every sane, sober, and otherwise sensible reader be asking: does any evidence exist showing that these drugs are effective, at least? Read on.
US Federal Vaccine Mandate Loses BIG in Court: US Government Legal Team Cannot Show Covid Vaccines Effective or Reduce Transmission
In the matter of the STATE OF MISSOURI, et al., (Plaintiffs) vs. JOSEPH R. BIDEN, JR., in his official capacity as the President of the United States of America, et al., (the Defendants), the court held that vaccines mandate are "likely an unlawful promulgation of regulations”, that "the Court’s duty is not to “rubber-stamp” administrative decisions devoid of reasonableness,” and pointedly:
In general, the overwhelming lack of evidence likely shows (the Defendant) had insufficient evidence to mandate vaccination on the wide range of facilities that it did. Looking even beyond the evidence deficiencies relating to the specific facilities covered, the lack of data regarding vaccination status and transmissibility — in general— is concerning. Indeed, (the Defendant) states that the “effectiveness of the vaccines[s] is currently unknown”.
Before our analysis on the implications of this legal decision, also see this report from THE LANCET Infectious Diseases – Transmissibility of SARS-CoV-2 among fully vaccinated individuals – published in January 2022, and note the highlighted portion of a screenshot from this report attached below, as follows:
This study showed that the impact of vaccination on community transmission of circulating variants of SARS-CoV-2 appeared to be not significantly different from the impact among unvaccinated people.

Figure 5: the Lancet (January 2022) – Transmissibility of SARS-CoV-2 among fully vaccinated individuals
Collectively, these refute the validity of claims that there is justification for ‘Proof of Vaccination’ edicts (vaccine passports and mandates) to reduce transmission.
Why the FDA’s ruse? Under US law, everyone has ‘right to refuse’ an Emergency Use Authorized (EUA) product.
When the FDA licenced Pfizer-BioNTech's Comirnaty COVID-19 vaccine on August 23, 2021, its approval was accompanied by a series of confusing documents and equally confusing public statements.
As I noted earlier, one such confounding statement (Letter One - footnote 8) reads as follows:
The licensed vaccine has the same formulation as the EUA-authorized vaccine and the products can be used interchangeably to provide the vaccination series without presenting any safety or effectiveness concerns. The products are legally distinct with certain differences that do not impact safety or effectiveness.
The FDA provided no explanation as to how the licensed Comirnaty vaccine and the Pfizer-BioNTech EUA vaccine could “be used interchangeably” despite having “certain differences” that make them “legally distinct.”
There are key legal differences between fully licensed vaccines and those authorized under a FDA EUA. EUA products are considered experimental under U.S. law. This means they cannot be mandated, and everyone has the right to refuse such vaccines without consequences.
Under US federal law, no human being can be forced to participate in a medical experiment. Under 21 U.S. Code Sec.360bbb-3(e)(1)(A)(ii)(III), “authorization for medical products for use in emergencies,” it is unlawful to deny someone a job or an education because they refuse to be an experimental subject.
This is also made clear in the FDA fact sheet provided to patients receiving any Pfizer COVID-19 vaccine. It states:
Under the EUA, it is your choice to receive or not receive the vaccine. Should you decide not to receive it, it will not change your standard medical care.
However, U.S. law does allow employers and schools to require students and workers to take licensed vaccines.
EUA products can’t be used once fully licensed product becomes available
Another key difference between fully licensed and EUA vaccines in the US is that, under the 2005 Public Readiness and Preparedness Act (PREP Act), EUA vaccines are accompanied by a far-reaching liability shield that protects all parties involved with the product from lawsuits.
At this time, the Pfizer Comirnaty vaccine may have no liability shield, making it subject to product liability laws that allow those injured by it to potentially sue for damages, although Pfizer asserts that the vaccine is protected in the US under the PREP Act as well.
When the US Centers for Disease Control and Prevention includes a fully licensed vaccine on its recommended vaccination schedule, the vaccines similarly enjoy generous liability protections, but those protections are not as complete as under the PREP Act[i].
The FDA fact sheet states:
This EUA for the Pfizer-BioNTech COVID-19 Vaccine and COMIRNATY will end when the Secretary of HHS determines that the circumstances justifying the EUA no longer exist or when there is a change in the approval status of the product such that an EUA is no longer needed.
This appears to contradict black-letter law in the US — defined as well-established legal rules in addition to well-established case law.
In this case, an EUA is considered illegal and invalid if there is a fully licensed alternative available. This appears to be the case with Pfizer’s licensed Comirnaty while its EUA Pfizer-BioNTech is still on the market.
As stated by Children’s Health Defense (CHD) in its lawsuit against the FDA and Dr. Janet Woodcock, acting commissioner:
The black letter law is clear. There can be no biologic license approved to a medical product for diagnosing, preventing or treating COVID-19 if there is also still an Emergency Use Authorization for the same medical product serving the same purpose.
In another CHD lawsuit, pertaining to mask mandates for school children issued under an EUA, CHD President Mary Holland, co-counsel on the case, stated that “[i]t is black-letter law that EUA devices … cannot be mandated at all.”
Still, most media outlets refer to COVID vaccine mandates as necessary if not inevitable, based on a narrative which attempts to lead the public into believing the COVID vaccines have been fully licensed.
The same media narratives, such as a USA Today “fact check,” also claim the Comirnaty and Pfizer-BioNTech vaccines are the same.
CHD though, in its lawsuit against the FDA, argues that Comirnaty’s licensure was a classic “bait and switch,” and that there is no legal basis to retain the EUA status for other COVID vaccines once the FDA has fully licensed a COVID vaccine.
A recent lawsuit filed by Arizona’s attorney general against the Biden administration over its vaccine mandates made a similar argument:
…the whole point of the mandates is to deny any such ‘option’ to those governed by them. Notably, only the Pfizer vaccine has received [U.S. Food and Drug Administration (FDA)] approval, and none of the stock of it in the U.S. is actually the FDA-approved version (and instead is entirely under the EUA label subject to the EUA-mandated conference of choice).
Do vaccines labeled ‘Comirnaty’ even exist in the US?
These issues came to a head in the order issued November 12, 2021 in Doe et al. v. Austin, U.S. Federal District Judge Allen Winsor of the U.S. District Court for the Northern District of Florida denied a preliminary injunction requested by 16 service members against the U.S. Military’s COVID vaccine mandate. A hearing is scheduled for September 14, 2022.
As recognized by the judge, “[u]nder the EUA statute, recipients of EUA drugs must be ‘informed … of the option to accept or refuse administration of the product.”
The judge further noted that regarding the administration of an EUA product to members of the armed forces, such a right of refusal may be waived only by the president.
The US Department of Defense (DOD) “acknowledges that the president has not executed a [waiver], so as things now stand, the DOD cannot mandate vaccines that only have an EUA.”
Judge Winsor also pointed out that “DOD’s guidance documents explicitly say only FDA-licensed COVID-19 vaccines are mandated.”
While this would be applicable to the Comirnaty vaccine, the judge noted “the plaintiffs have shown that the DOD is requiring injections from vials not labeled ‘Comirnaty.’ Indeed, defense counsel could not even say whether vaccines labeled ‘Comirnaty’ exist at all.”
The judge also noted that the DOD “later clarified that it was mandating vaccines from EUA-labeled vials,” adding that “[i]n the DOD’s view, this is fine because the contents of EUA-labeled vials are chemically identical to the contents of vials labeled ‘Comirnaty’ (if there are any such vials).”
The judge found this argument “unconvincing,” stating that “FDA licensure does not retroactively apply to vials shipped before BLA approval.”
He further noted that EUA provisions suggest “drugs mandated for military personnel be actually BLA-approved, not merely chemically similar to a BLA-approved drug,” not just in terms of labeling, but also in terms of being produced at BLA-compliant facilities.
As the judge stated, “there is no indication that all EUA-labeled vials are from BLA-approved facilities,” adding that “the DOD cannot rely on the FDA to find that the two drugs are legally identical.” However, the judge’s acknowledgment that “the DOD cannot mandate vaccines that only have an EUA” is significant for two reasons.
One reason pertains to the difference in ingredients and manufacturing process between Pfizer’s EUA vaccine and the approved Comirnaty vaccine, and the other pertains to the legal difference between a fully licensed vaccine and an EUA vaccine.
Summary:
It is a sad reflection of the state of federal regulatory agencies that actively harm and discredit themselves to serve the interests of pharmaceutical interests to the detriment of the public they are supposed to serve. It is misleading to tell the public that the Pfizer Covid vaccine has been licensed in the US, implying that an FDA-approved/licensed Pfizer Covid vaccine is currently being offered in the United States, when it is not, or that it has been “approved” by Health Canada, when it has not.
To restate: the FDA has licensed and approved "a" Pfizer Covid Covid-19 vaccine. The distinctive brand-name for the FDA-approved vaccine is "Comirnaty." Do not, however, expect Pfizer to sell, distribute, or make generally available the Comirnaty vaccine in the U.S. This is because Pfizer has not obtained legal immunity for the Comirnaty vaccine.
If Pfizer were to sell, distribute, or make available the Comirnaty vaccine in the U.S., then Pfizer could be held legally responsible for the adverse health outcomes caused by Comiraty, which, unlike child vaccines in the US, is subject to normal product liability laws. Because of this fact, expect the FDA-approved Comirnaty vaccine to remain unavailable as long as Pfizer remains exposed to product liability suits brought by anyone injured by Comirnaty.
Pfizer's other Covid vaccine, the BioNTech brand, enjoys complete legal immunity in the U.S. market but has not obtained FDA approval. The BioNTech vaccine is being administered under the Emergency Use Authorization ("EUA") and enjoys complete legal immunity under the PREP Act. EUA is a legal end-run around the FDA approval process made possible by the "pandemic."
Echoing neoclassical economic theory, the "show-me-the-incentive-and-I-will-show-you-the-outcome" of the Comirnaty/BioNTech distinction is of course: (1) Pfizer's FDA-licensed and approved Comirnaty shot is not available in the United States; and (2) Pfizer's unlicensed and unapproved (but legally authorized for emergency use) BioNTech shot is abundantly available and will remain abundantly available. The reason? Financial incentives and disincentives.
If Pfizer were to sell or distribute Comirnaty in the U.S., Pfizer would face product liability lawsuits. Pfizer would be held responsible for the injuries Comirnaty has caused. Legal responsibility and liability for injury = economic disincentive to supply = lack of supply.
Pfizer’s BioNTech shot, however, enjoys complete and total immunity from any and all death, damages and other injuries that they cause. Pfizer-BioNTech's immunity shield means that Pfizer has no risk and no downside for selling it in the U.S. No legal responsibility and no liability for injury and death = economic incentive to sell and supply = abundant supply.
One would think that a government regulator, after going through a purportedly arduous expedited approval process, would likely be indignant that its regulatory subject was withholding from the public the only licensed and approved anti-pandemic drug, in the middle of a "pandemic".
Not so the FDA. It falsely implies that the Pfizer vaccine being sold and distributed in the U.S. is FDA approved when it is not. The FDA claims that the two Pfizer Covid vaccines are the same, although "legally distinct." Legally distinct means that if you are injured or killed by the abundantly available BioNTech vaccine, you will have no legal recourse against Pfizer.
If Comirnaty were available in the US, or if it had really been “approved” in Canada, and it injured you, you could sue Pfizer and win.
Neither the FDA or Health Canada, which can treat the FDA as a foreign regulatory authority when it authorizes a designated Covid-19 Drug as a “New Drug” (meaning definitively a drug of unknown safety/efficacy) under to Division 8 of the Food and Drug Regulation, will tell you this.
It almost seems as though they needed a way make an unwary public think “a” Pfizer-BioNTech Covid-19 vaccine had been licensed/approved, while still enjoying a full liability shield/EAU for the BioNTech labeled version of the drug with the “same formulation” (see Letter One – page 2) still in use.
If so, the FDA met this objective by issuing two letters to Pfizer-BioNTech on August 23, 2021, and then politicians, the media, and public health officials blurred the lines between these already blurry two letters.
Health Canada performed their Division 8 “bait and switch” less than a month later on September 15, 2021. Why? To confuse and mislead the public? If so, what was their real intent? So that these New Drugs, of undetermined efficacy and safety (especially longer term), could then be plausibly mandated by governments and employers, and also marketed to children?
In Part Three of this Investigative Report we delve into what is known about the actual epidemiology of Covid-19 (versus The Covid Scare), and what was known as early as October 2020, at the very least.
To prepare yourself for what we will discussing in Part Three, since many I think will find it rather strong medicine, I strongly suggest you view the following two short YouTube videos from the very early days of the “pandemic”.
Dr. Ngozi Ezike MD, Director Illinois Department of Public Health | How COVID Deaths are Classified | April 17, 2020.
Next, Montana physician Dr. Annie Bukacek discusses | How COVID 19 death certificates are being manipulated | April 6, 2020.
Final proof? On February 7, 2022, the US CDC and HHS announced that they are working to recalculate Covid hospitalizations in the U.S. The CDC and HHS are:
Asking hospitals to report numbers of patients who go to the facility because they have Covid-19 and separate those from individuals who go in for other reasons and test positive after being admitted.
This represents de facto admission that Covid-19 stats on mortality and morbidity were manipulated to carry out an agenda from the very beginning. Why?